

Should we Change our notion of Clavicle fracture treatment?
Although most conservatively treated midshaft clavicular fractures were traditionally thought to unite,recent clinical evidence suggests that nonunion after fractures is rather common. Unfortunately, non-union often causes pain and impaired function of the shoulder girdle.
Recent literature is challenging the traditional belief that midshaft clavicle fractures
uniformly heal without functional deficit. This paradigm shift is supported by several prospective studies by members of the Canadian Orthopaedic Trauma Society, who reported higher nonunion rates and functional deficits after nonsurgical treatment of midshaft clavicle fractures when compared with internal fixation.

Recent studies have shown that long-term results from conservative, or non-operative, management of clavicular fractures are not as favourable as previously considered:
42% of people still had sequelae at 6 months in one study. The same study suggests the exploration of alternative treatment options, including surgery, for certain clavicular fracture types.[7]
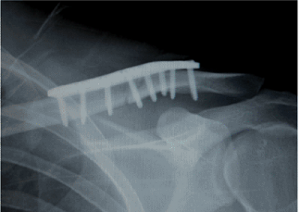
A recent multicentre randomised controlled trial in Canada showed that displaced clavicle shaft fractures treated by surgical plate fixation had improved functional outcome and a lower rate of malunion and nonunion when compared with nonoperative treatment at one year.
Another study into nonoperative treatment of displaced mid-clavicular shaft fractures detected significant residual deficits in shoulder strength and endurance.
Indications for acute surgical treatment may include younger, active patients with clavicle shortening greater than 1.5 to 2 cm, significant cosmetic deformity, or multiple-trauma situations.
The Clavicle has many functions including acting as strut to hold the scapula away from body, serves as attachment for muscles, provides protection for underlying blood vessels and nerves. It also helps in transmitting the forces to the scapula.
The clavicle also assists with the external, upward, and posterior rotation of the scapula. This has been supported by number of Cadaveric and clinical studies.
Upward scapular rotation elevates the lateral acromion, whereas its posterior tilting elevates the anterior acromion; thus, by influencing scapular motion, the clavicle may assist the motion of the glenohumeral joint and decrease subacromial pressure
Shoulder dyskinesia affects surrounding muscles of scapula and the entire kinematic chain from the trunk to the upper extremity.Clavicular discontinuity changes the shoulder girdle kinematics, resulting in decreased external rotation, upward rotation, and posterior tilting of the scapula. This in turn can lead to secondary impingement of shoulder.